
SUNAO FUJITA
Clinical history:
A 16-year-old, thoroughbred gelding presented with a slow growing mass in the left ventral thoracic/axillar region, extending into deep tissue (Figure 1). The mass was firm and non-mobile and had been present for six months, but had not changed in size.

Cytology:
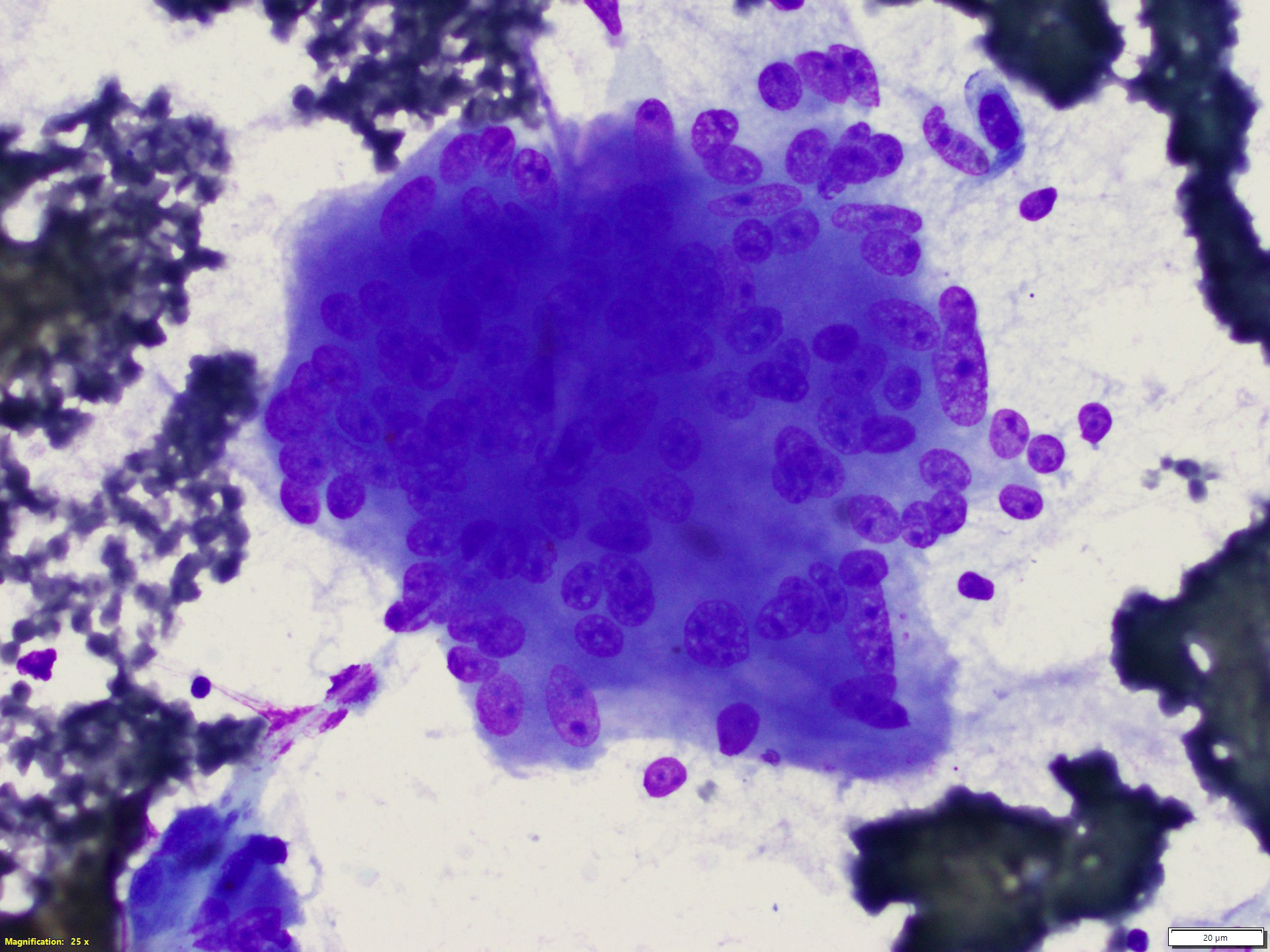
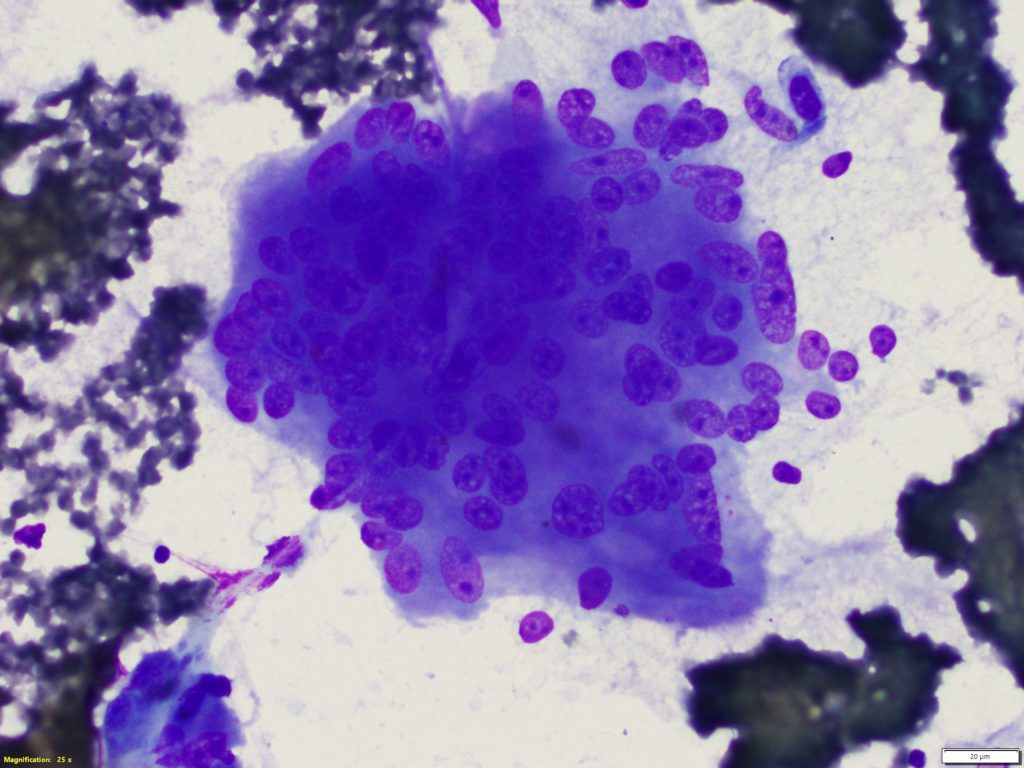
The smears were of high cellularity, predominantly composed of spindle cells with moderate numbers of macrophages. The spindle cells were sometimes arranged in variably sized aggregates with small amounts of associated eosinophilic extracellular matrix. Their nuclei contained finely stippled chromatin with single to multiple nucleoli. They had moderate amounts of basophilic cytoplasm and showed moderate anisocytosis and anisokaryosis.
There were occasional multinucleated giant cells – up to 100 nuclei (Figure 2). The macrophages frequently contained phagocytized haemosiderin and/or hematoidin crystals. Given the marked spindle cell proliferation with moderate atypia and the occasional multi-nucleated giant cells, a top differential was a giant cell tumour of soft parts.
Histology:
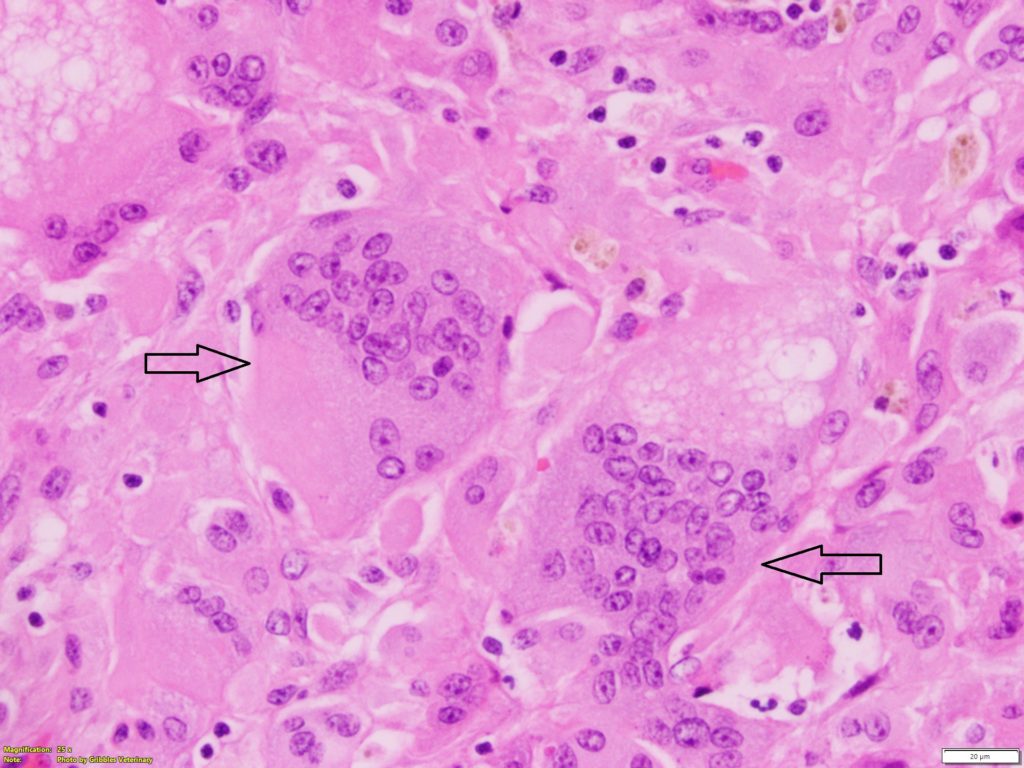
Surgical excision for histopathology was performed two-months after the cytologic examination. Infiltrating the subcutis to the lateral margins of the tissue were proliferations of spindle cells admixed with small numbers of inflammatory cells (macrophages, lymphocytes and plasma cells). The spindle cells had moderate anisocytosis and anisokaryosis, and were often multinucleate with three mitotic figures per high power field (400x) (Figure 3). Some of the neoplastic cells and macrophages contained phagocytized haemosiderin.
Diagnosis:
Giant cell tumour of soft parts.
Discussion:
The terminology/ classification, cellular origin, and microscopic criteria of giant cell tumour of soft parts (GCTSP), have been historically confusing in veterinary medicine. The histogenesis and origin for GCTSP remains controversial and uncertain.
Initially, this neoplasm was reported in humans and cats. It was referred to as malignant giant cell tumour of tendon sheath, and considered a malignant counterpart of benign giant cell tumour of tendon and tendon sheath (since tendon/tendon sheath appeared to be original sites of the neoplasm)1. However, further studies revealed that GCTSP can be seen in different locations and is regarded as a distinct entity with a different origin.
GCTSP is reported in many domestic species (horses, dogs, cats, etc.) as well as humans. In humans, superficial and deep forms have been described, based on the localization and growth pattern. In veterinary medicine, the deep form has been observed mostly in cats and dogs, whereas horses commonly have the superficial form.2
The deep forms typically involve fascia and skeletal muscle with high metastatic potential, and neoplastic cells show marked atypia with high mitotic rate. Conversely, the superficial forms are seen within subcutaneous tissue with minimal atypia and low mitotic rate, and rarely metastasize.2 Given the difference in locations, biologic behaviours and morphologic features, the superficial form (benign type) has been classified in the category of fibrohistiocytic tumours. The deep forms (malignant type) have been referred to as anaplastic sarcoma with giant cells, and categorized under undifferentiated/unclassified sarcomas. This also includes a group of sarcomas with various cellular origins, which may represent
anaplastic variants of different sarcomas (fibrosarcoma, myofibroblastic fibrosarcoma, liposarcoma, leiomyosarcoma, rhabdomyosarcoma, synovial cell sarcoma histiocytic sarcoma, etc.).1,3
In horses, GCTSP is a rare cutaneous neoplasm (approximately 1% of cutaneous neoplasms).4 The neoplasms are commonly seen in old horses (>10 years) and occur as solitary, raised, firm masses that may be ulcerated. They are predisposed to be present on the hind-limbs, but have also reported on the thorax, shoulder, abdomen, muzzle, and jugular groove.5
Cytologically, they are characterized by variable cellularity and a proliferation of spindle cells, with the presence of multinucleated giant cells that have multiple nuclei (up to 100 nuclei) and abundant basophilic tapered cytoplasm. An infiltrate of mixed inflammatory cells (neutrophils, macrophages, lymphocytes, and plasma cells) is commonly seen with evidence of chronic haemorrhage (e.g. macrophages with phagocytized RBCs or RBC breakdown products).
While the histogenesis of GCTSP is unclear, the majority of cases revealed positive immunohistochemical staining for vimentin, which supports mesenchymal origin.1
The metastatic potential is generally low and surgical excision is curative in most cases. However, local recurrence has been reported in the case of incomplete or minimal excision.5 In the present case, no overt evidence of neoplasm recurrence has been seen 15-months after surgery.
Thank you to Alex Fowler, Veterinary Associates Equine for this interesting case.
References:
1. Cian, F., Whiteoak, S., Stewart, J. A case of giant cell tumour of soft parts in a horse. Vet Clin Pathol, 45:501-504. 2016.
2. Zimmerman, K., Almy, F., Saunders, G. et al. An unusual case of giant cell tumor of soft parts in an America Warmblood horse. Open Veterinary Journal, 9:44-48, 2019.
3. Gross, T.L., Ihrke, P.J., Walder, E.J., et al. Other Mesenchymal Tumors. In: Skin diseases of the dog and cat, clinical and histopathologic diagnosis 2nd ed, pp. 806-810, Blackwell Science Ltd., Oxford. 2005.
4. Schaffer, P.A., Wobeser, B., Martin, L.E., et al. Cutaneous neoplastic lesions of equids in the Central United States and Canada: 3351 biopsy specimens from 3272 equids (2000-2010). J Am Vet Med Assoc. 242:99-104, 2013.
5. Walton, R.M., Cowell, R.L., Valenciano, A.C. (2021): Cytology of Cutaneous and Subcutaneous Lesions. In: Equine hematology, cytology, and clinical chemistry 2nd ed, pp. 161-193, Wiley Blackwell, Hoboken.