
HANIA KLOBUKOWSKA
Feline infectious peritonitis (FIP) is a disease not uncommonly seen throughout New Zealand. It is caused by feline enteric coronavirus (FECV) which exists as two pathotypes: the ‘ubiquitous enteric biotype’ and the ‘virulent biotype.’
The enteric biotype has a prevalence that approaches 100%, especially in multi-cat households, and mainly causes a self-limiting diarrhoea. The virulent biotype causes FIP in cats. FIP develops in cats from mutations in an already present avirulent FECV. Although the prevalence of FECV in cats is high, only a very small proportion of these will go on to develop FIP and it is thought that the already present virus undergoes a mutation which allows it to replicate internally in monocytes and cause disease. There may also be genetic factors, in addition to having the mutant FECV, that predispose certain cats to the development of disease.
Diagnosis:
Diagnosing FIP can be challenging, as currently there are no reliable tests that can distinguish between the enteric and virulent biotypes of FECV. Veterinarians must employ a number of diagnostic tests and clinical nous to increase or decrease their levels of suspicion when dealing with suspect FIP cases. It is also important to note, that most existing diagnostic tests cannot differentiate between the avirulent and virulent biotypes of FECV.
The following information may be useful in navigating such cases.
Risk factors:
FIP is most commonly seen in young cats (6-months to 2-years old) that are purebred and male. Certain breeds are also at a higher risk e.g. Birmans and Ragdolls. Note that these rules are not exclusive, as we do see FIP in domestic breeds and older patients as well.
Clinical presentation:
The archetypical presentation of FIP is that of a cat that presents with a peritoneal and/or thoracic protein-rich effusion. These cats often have other non-specific clinical findings such as inappetance/anorexia, vomiting, diarrhoea, weight loss etc. Other clinical presentations can include the more diagnostically challenging ‘non-effusive’ form of FIP, where internal organs are affected without an obvious exudate.
On necropsy, many of these cases do in fact have evidence of an effusion, however it is often minimal and so would have been difficult to collect ante-mortem. Any young cat that presents with neurological or ocular symptoms should be investigated for FIP. There are also some uncommon manifestations of the disease, such as solitary mural colonic or ileocecocolic masses – this is an example of a localised presentation of FIP.
Haematology and biochemistry:
Common alterations include a mild to moderate regenerative or non-regenerative anaemia, lymphopaenia and hyperproteinaemia (due to elevated globulins). There may also be derangements in other parameters which will likely reflect organ damage (e.g. azotaemia, elevated liver enzymes etc.).
Albumin to globulin ratios (A:G ratio) may be of high diagnostic value, as levels >0.8 make FIP highly unlikely.
Effusion analysis:
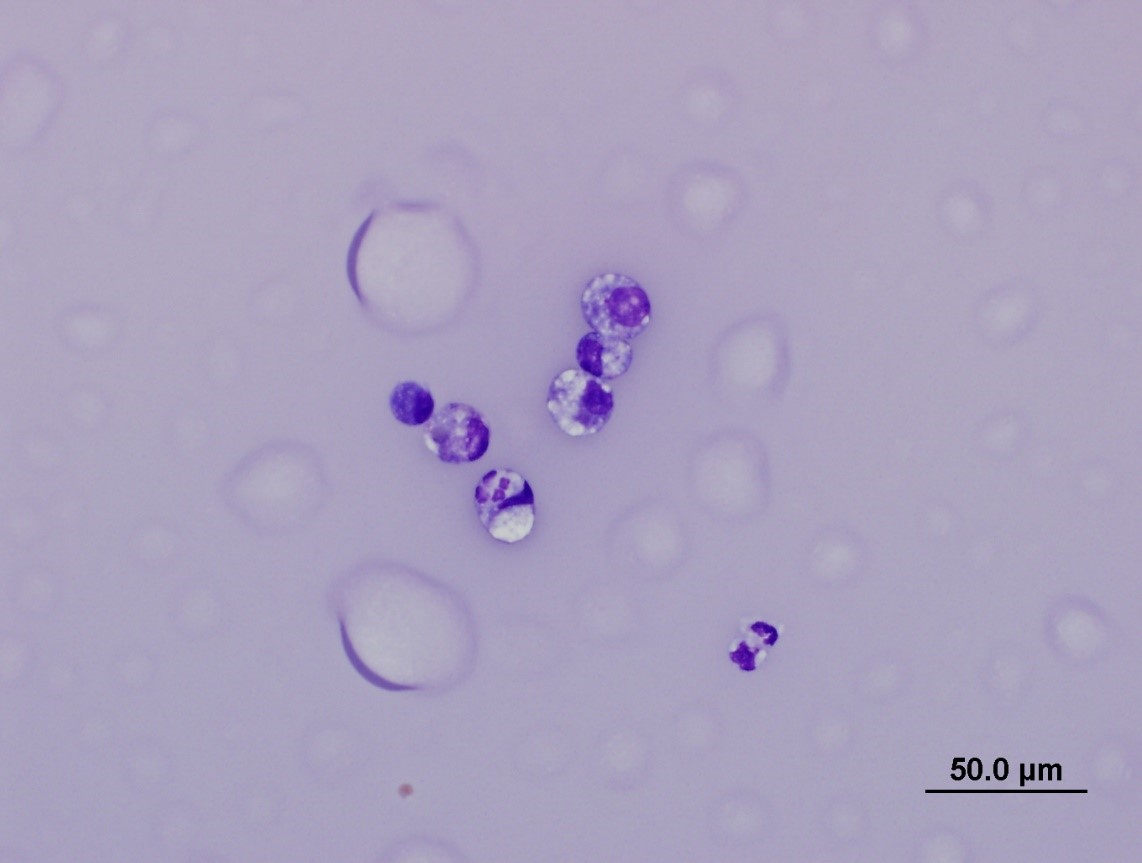
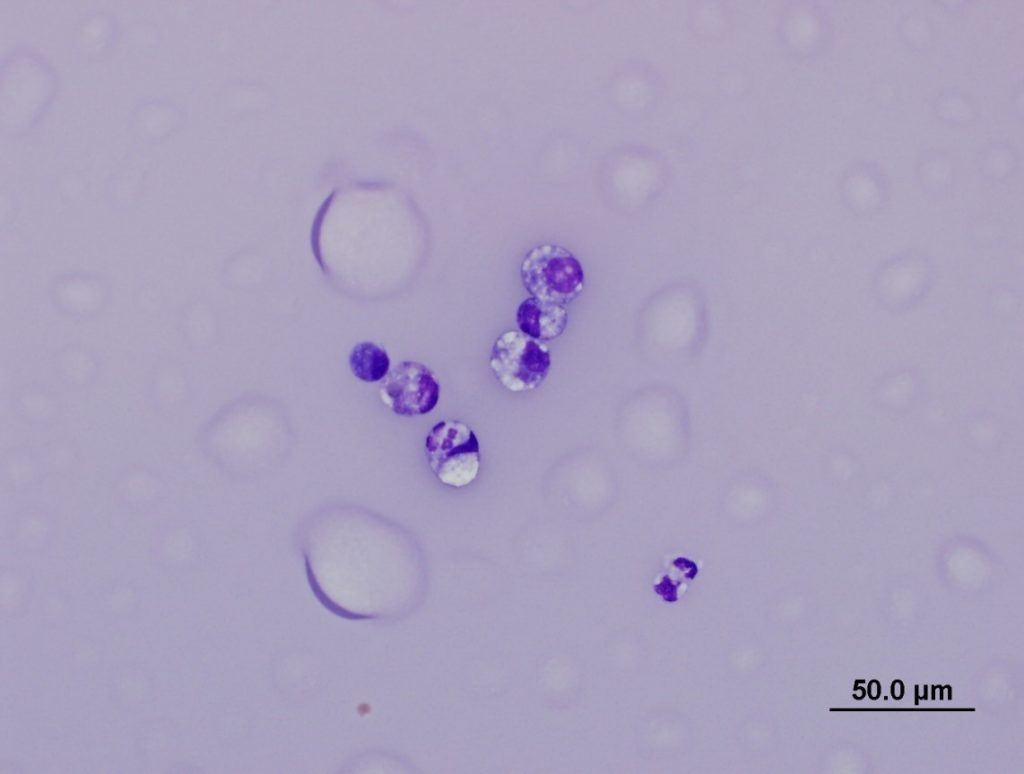
FIP effusions are of high diagnostic value and are typically high protein with low cellularity. Cytologic examination of these usually reveals a dominance of macrophages and neutrophils on a very proteinaceous background (see Figure 1). Cytological examination of effusions can also help rule out other differentials for effusive disease (such as septic processes or neoplasia).
The A:G ratio can also be measured in effusions and similar to the biochemistry interpretation, levels >0.8 make FIP highly unlikely.
Serology:
Serum evaluation of antibody levels does not differentiate between the avirulent and virulent biotypes of FECV. Most cats have circulating antibodies to FECV and as mentioned, only a small proportion of infected cats go on to develop FIP. The presence of antibodies (even high titres) may hence be of limited diagnostic value, furthermore, approximately 10% of cats with FIP can be seronegative, especially if they are end-stage.
FECV antibodies can also be examined in effusions however the diagnostic value of this is similarly low as serum evaluation.
Assessing FECV antibodies may be of value in assessing disease status in multi-cat households for disease prevention and/or control.
RT-PCR:
Gribbles Veterinary has the capacity to detect FECV antigen via RT-PCR in effusions. This test does not differentiate between the avirulent and virulent FECV biotype.
When performed on effusions, the sensitivity and specificity is high according to a number of reported studies. Detection of high viral loads in an effusion has high diagnostic value in a cat suspected of having FIP. Very occasional false-positive results can occur so, as previously emphasised, this test should not be used in isolation.
The RT-PCR can also be performed on fresh tissues (e.g. aspirates from lymph nodes or other affected organs) however the diagnostic sensitivity and specificity is not as high as using fluid. RT-PCR on fresh tissues may be a more practical option in cases that are not clinically effusive. Alternatively RT-PCR can be attempted on peritoneal lavage samples from cases that are not clinically effusive however the diagnostic accuracy of this is not well established.
Histology/immunohistochemistry (IHC):
Immunohistochemical detection of FECV antigen within characteristic histopathologic tissue lesions is considered the gold standard for FIP diagnosis. Currently Gribbles Veterinary has the capacity to perform histopathology in such cases however IHC can only be performed at an external overseas laboratory. In most cases histopathology is performed on post mortem samples as it is an invasive procedure to do in a live, sick cat.
Histopathology of FIP lesions is generally characteristic in representative samples and is characterised by a vasculitis/phlebitis with associated pyogranulomatous and/or lymphoplasmacytic cellular infiltrates. Distribution of lesions varies amongst animals, however the most common sites to see pathology are the peritoneum/mesentery, kidneys and lymph nodes, and a full set of tissues should always be sampled to increase diagnostic accuracy. Any cat with neurological and/or ocular symptoms should have those corresponding organs assessed histologically.
Conclusion:
Ante-mortem diagnosis of FIP can be a challenge to even the most experienced clinician, and it must be reiterated that no single ante-mortem test is perfectly accurate. Given that the prognosis for FIP is poor without treatment, and may end in euthanasia, a number of tests should be employed so the clinician can arrive at a relatively certain diagnosis before committing to further decisions about patient management.
References
- Felten S and Hartmann K. Diagnosis of Feline Infectious Peritonitis: A Review of the Current Literature. Viruses 2019, 11, 1068
- Kipar A and Meli ML. Feline Infectious Peritonitis: Still an Enigma? Vet Pathol 2014, 51(2), 505-526