

MICHAEL HARDCASTLE
Clinical history:
A sixteen year old Domestic Short Hair cat presented with a two-week history of severely crusted, erythematous and painful skin around the nail beds of both forelimbs and the caudolateral aspects of the pinnae. (Figures 1-3). The cat’s skin was otherwise unremarkable, and the only other clinical findings were lean body condition and pyrexia. There was no prior history of topical or systemic medication.



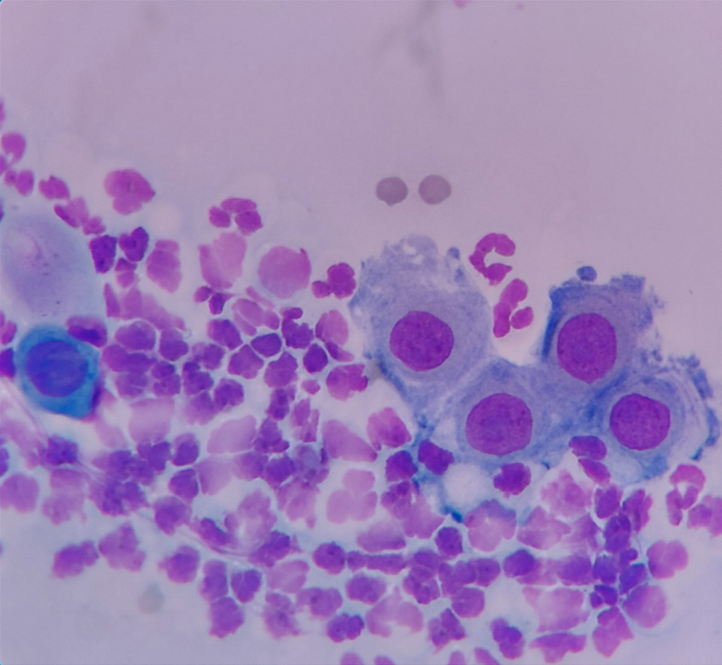
In-house haematology and biochemistry testing reportedly showed moderate neutrophilia and a moderate increase of globulins. In-house cytology of the crusts showed neutrophils and individualised keratinocytes (Figure 4).
Skin biopsies were collected from the left and right fore dew claws and the left and right pinnal margins.
Laboratory findings:
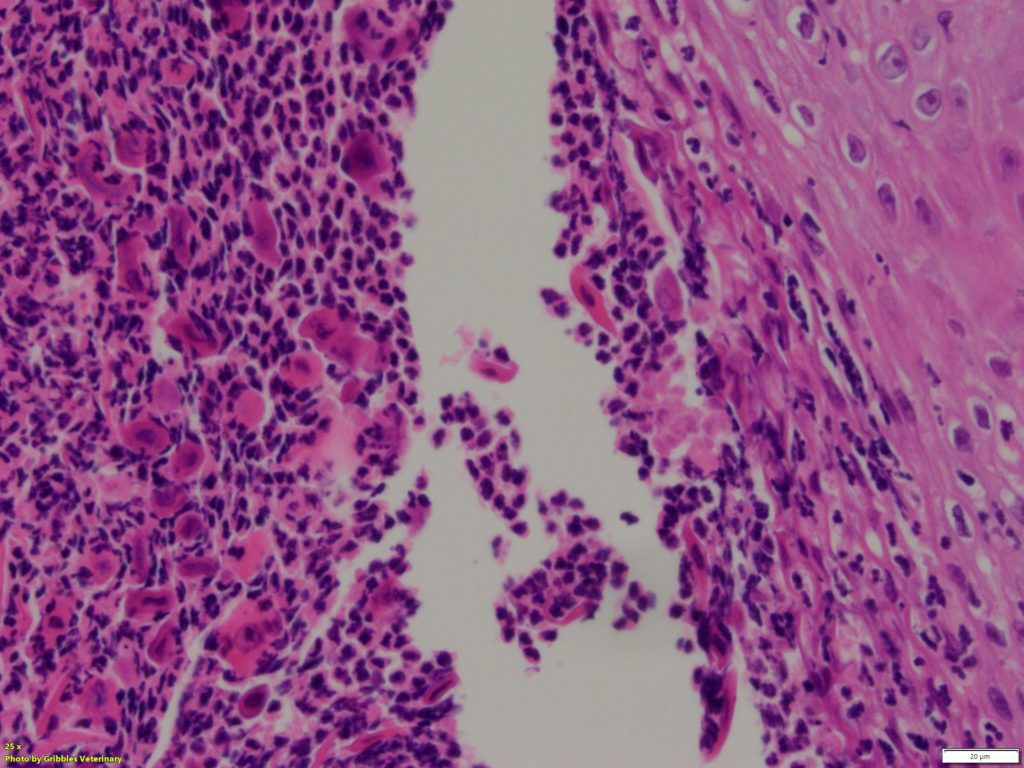
On histopathology these showed surface crusting and ruptured subcorneal pustules, with many variably necrotic neutrophils and acantholytic cells; these sometimes detached from the epidermis in a manner resembling a “crumbling brick wall”. (Figure 5). The dermis contained neutrophils, mast cells, lymphocytes, and plasma cells within variable oedema and fibrosis. Special stains showed scattered cocci in crusts and no fungi.
Diagnosis: Pemphigus foliaceus
Discussion:
Skin crusting and inflammation including acantholytic cells apparently arising from subcorneal pustules, is consistent with pemphigus foliaceus, a disease characterised by immune-mediated attack on epithelial adhesion molecules. The main differential diagnosis is a severe superficial infection (by bacteria or dermatophytes), which is difficult to completely rule out without intact pustules to check for microbes, since the sterile pustules of pemphigus can be invaded by microbes once ruptured. However, infectious acantholysis is considered rare and may be less severe than that in pemphigus.
Pemphigus foliaceus tends to be seen on the muzzle, planum nasale, perioral region, ear pinnae, nipples and distal extremities of cats. The pinnae and nail beds are the most frequently affected sites, with some cats presenting only with nail bed lesions. Sex or breed predilections have not been reported in cats. Most cats are middle-aged, although it can affect a wide age range. Methimazole and other drugs have been associated with pemphigus foliaceus-like disease as a drug reaction, and it has been associated with underlying thymoma in two cats, but in many cases of pemphigus the cause is unknown.
The prognosis for this disease in cats is quite good, with successful treatment options including prednisolone, chlorambucil or triamcinolone. This patient is reportedly responding very well to prednisolone.
Many thanks to Mary-Beth Dwyer, Franklin Veterinary Services, for submitting this interesting case and providing support to write this article.
References:
– Skin diseases of the Dog and Cat. 2nd edn. Pp. 13-18. Blackwell Science USA 2005
– Muller and Kirk’s Small Animal Dermatology 7th edn. Pp. 447-448 Elsevier USA 2013.
– Feline pemphigus foliaceus: original case series and a comprehensive literature review. BMC Veterinary Research 2019 15:22. https://doi.org/10.1186/s12917-018-1739-y