
CATHY HARVEY
Clinical history:
A four-year-old spayed female Staffordshire bull terrier presented after a one-week history of anorexia with vomiting and diarrhoea. She had been treated with antibiotics, anti-emetics, antacids and antiulcer medications. When the dog deteriorated (white gums and lethargic) further work-up was consented to by the owner.
On abdominal ultrasound, there was free fluid in the abdomen around a small intestinal lesion that was highly suspicious for a mass. The wall was severely thickened (measuring up to 1cm) and irregular. Mesenteric lymph nodes were all enlarged and hypoechoic. The rest of the abdominal lymph nodes were also enlarged. Stomach was filled with food. The remainder of the small intestines mildly thickened and hyperechoic omentum, early peritonitis. Liver, kidneys and spleen normal size and echogenicity. On an exploratory laparotomy a large thickened area of the jejunum was found. The mesenteric lymph node was enlarged. An end-to-end anastomosis was performed.
Diagnostic samples:
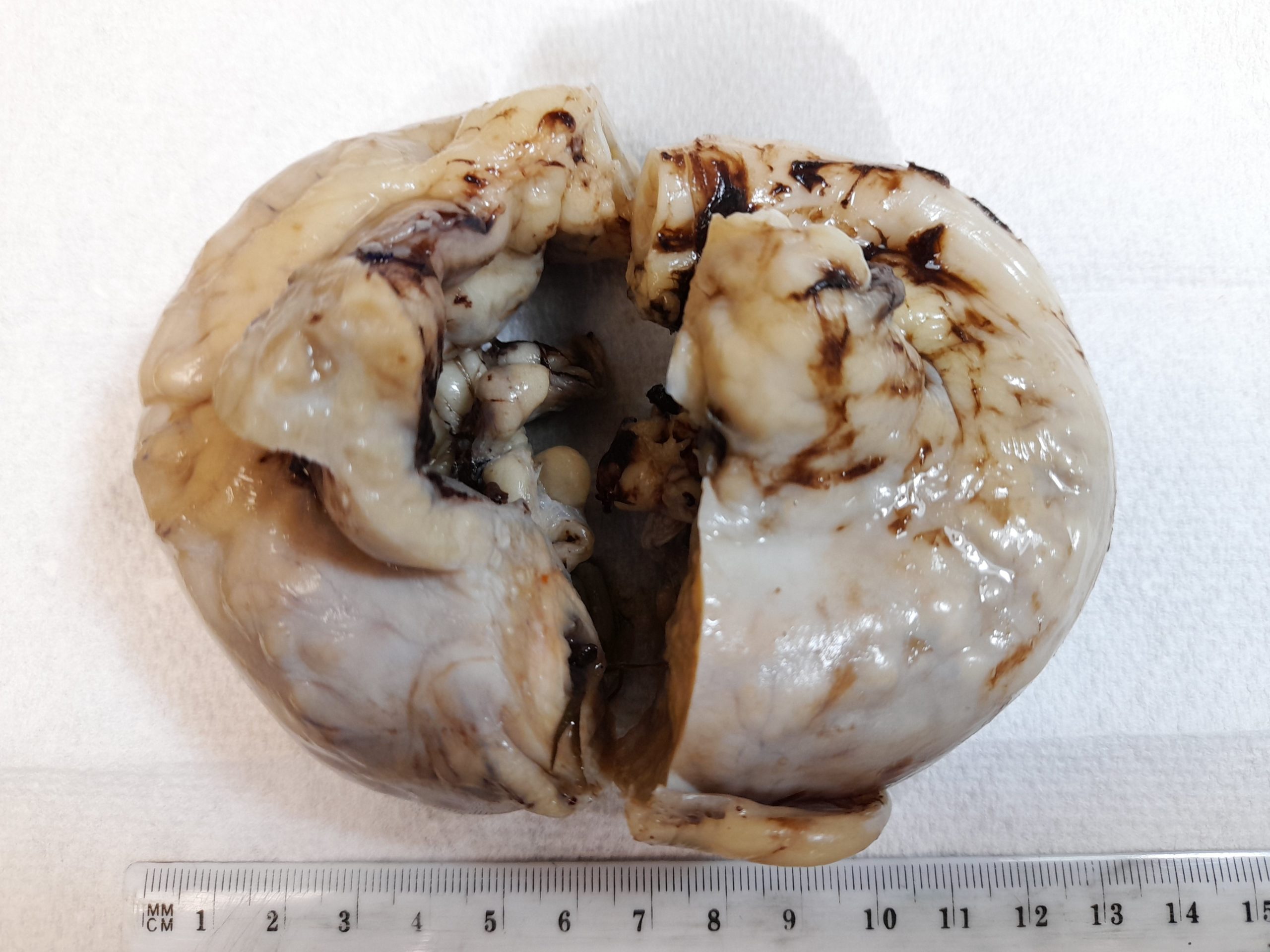
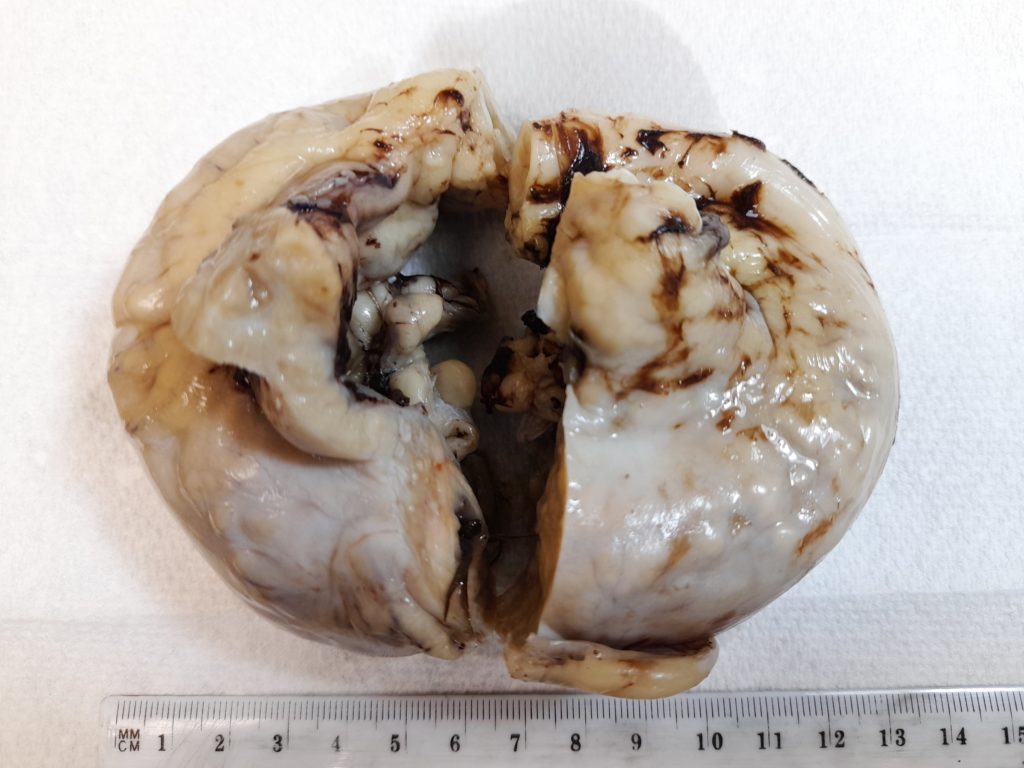
The mass tissue submitted to the laboratory for histopathology was a 240mm long section of intestine, and 20mm firm mass in the adjacent mesentery. See Figures 1 and 2.

Histopathology findings:
On histopathology the mucosa was ulcerated. Throughout the remainder of the wall of the intestine, and extending into the mesentery, there were multifocal to coalescing areas of numerous macrophages (epithelioid and multinucleate) and neutrophils, with areas of necrosis.
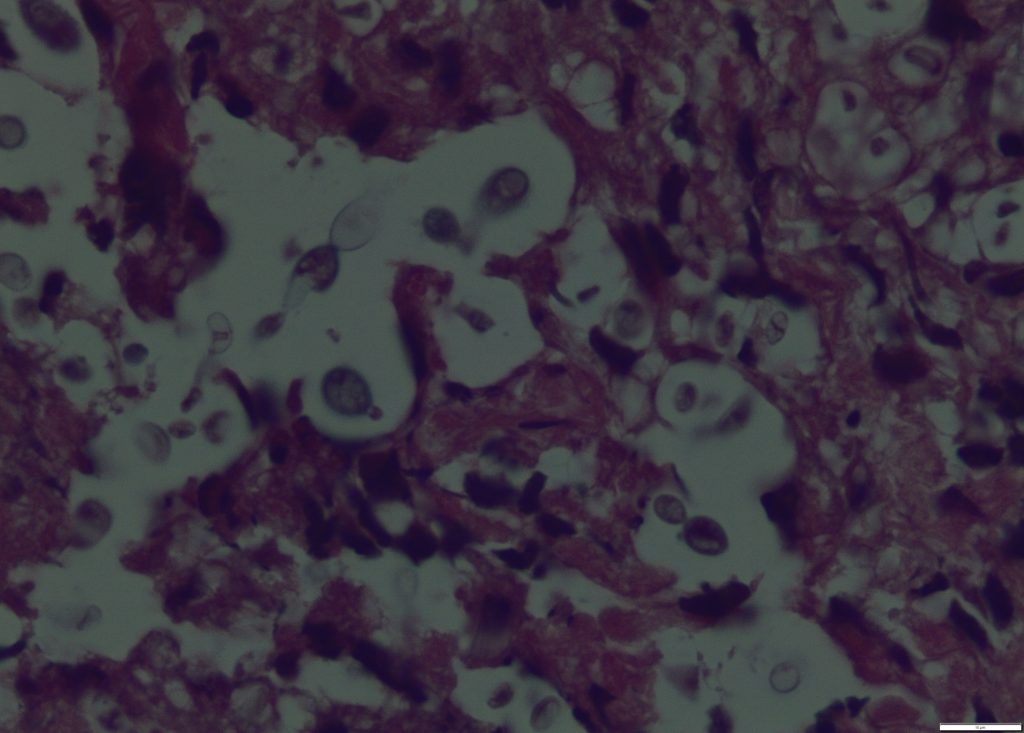
In the centres of the areas of necrosis and within the cytoplasm of the macrophages there were numerous PAS-positive narrow based budding yeasts, and rare hyphae/pseudohyphae (see Figure 3). The fungi and inflammation did not extend to the proximal and distal margins of the intestinal tissue but did extend to the serosal and mesenteric margins.
Histopathological diagnosis:
Pyogranulomatous transmural enteritis and peritonitis with intralesional yeasts.
Discussion:
Enteric fungal infections, especially with yeasts, are uncommon. Definitive diagnosis would require culture or PCR. DDX Candida spp. or possibly Cryptococcus spp.
Heavy fungal challenge, disruption of the normal flora, a primary local lesion, and/or lowered host resistance are probably required for establishment of mycotic disease in the gut. Spores are probably normally carried across the mucosa by macrophages, and only if host immunity is compromised in some way will they establish in the deeper tissues or become disseminated. Lesions occur anywhere in the gastrointestinal tract, including the fore stomachs of ruminants, and in the mesenteric lymph nodes. Clinical signs may be related to the location of the lesions, be non-specific, or entirely absent. Two primary types of lesions are produced: necrosis and haemorrhage or granulomatous inflammation. The most common organisms associated with alimentary tract mycoses are Zygomycetes (Mucor sp., Mortierella sp.), and rarely Aspergillus spp., Candida spp., and Histoplasma capsulatum.
Candida has been reported to uncommonly cause intestinal lesions such as these – usually in immunocompromised animals, or that have had previous antibiotics / GIT surgery. Candida spp. are commensals normally inhabiting the alimentary, upper respiratory, and lower urogenital tracts of mammals. They are opportunistic pathogens that can invade and colonise tissue when the patient is immune-compromised or there is disruption of the mucosal barrier.
Cryptococcus is an environmental yeast that (especially if immunocompromised due to neoplasia, diabetes mellitus, steroids) can cause infection, usually of the skin, respiratory tract, central nervous system and eyes. The yeasts are inhaled or inoculated from the environment (soil or bird droppings – especially pigeons, or Eucalyptus trees). Cryptococcosis is a zoonotic disease.
Many thanks to Dr Eckhard Stalmann from Veterinary Associates Takanini for submitting this interesting case. The dog is doing well post-surgery.
References:
Bradford K, Meinkoth J, McKeirnen K, Love B. Candida peritonitis in dogs: report of 5 cases. Veterinary Clinical Pathology 42:227-233, 2013.
Uzal FA, Plattner BL, Hostetter JM. Alimentary System—Mycotic diseases of the gastrointestinal tract. In: Jubb, Kennedy and Palmer (eds). Pathology of Domestic Animals 6th Edn. Pp 201-202. Elsevier Inc. USA, 2015.