
AMY WEEDEN
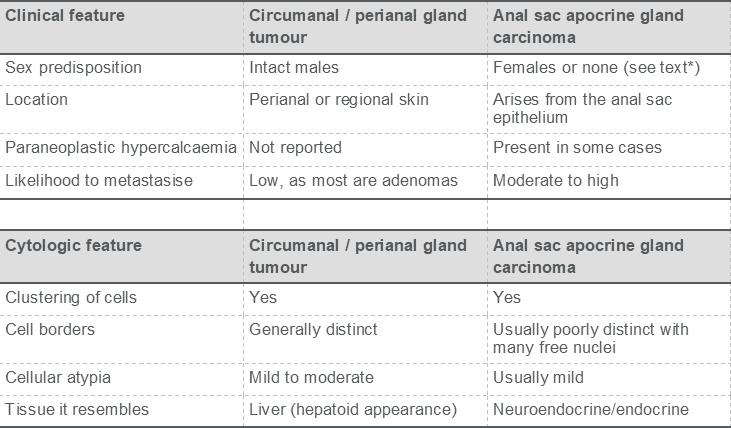
Perianal tumours are fairly common in dogs. Distinguishing between the two neoplasms, which are specific to this anatomic location, is often straightforward. However, if this is not the case, there are some clinical and cytologic differences that will usually provide a definitive diagnosis.
Circumanal gland tumours are also known as perianal gland tumours or hepatoid tumours, as the cells resemble hepatocytes microscopically. These tumors are androgen-responsive and usually found in intact male dogs, though they can be seen in either sex and in castrated/ speyed dogs.
Masses are usually found in the immediate perineal region, though they can also be seen in other locations in the caudal aspect of the dog (tail, prepuce, thigh, etc.). Most are benign, but circumanal gland carcinomas do rarely occur.
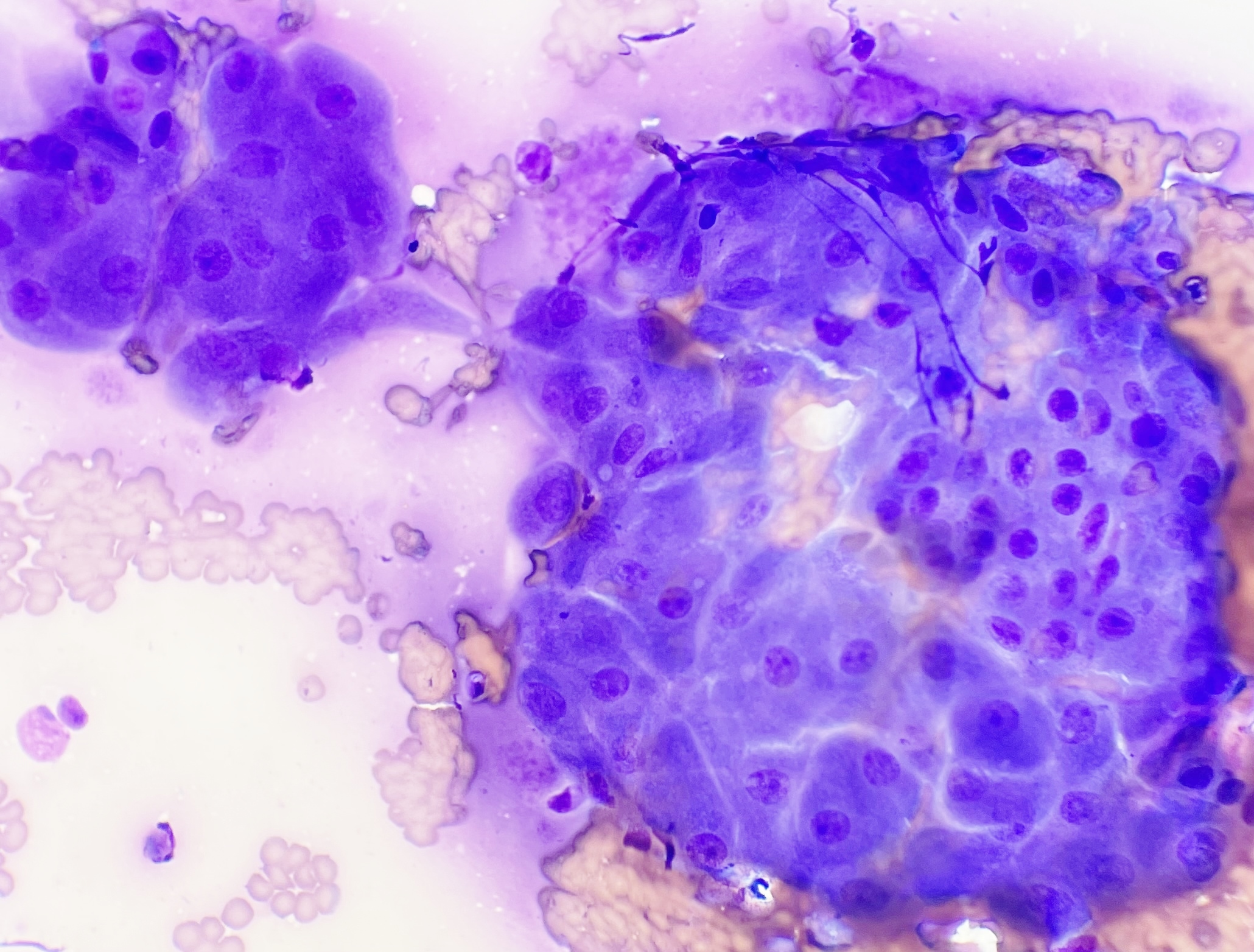
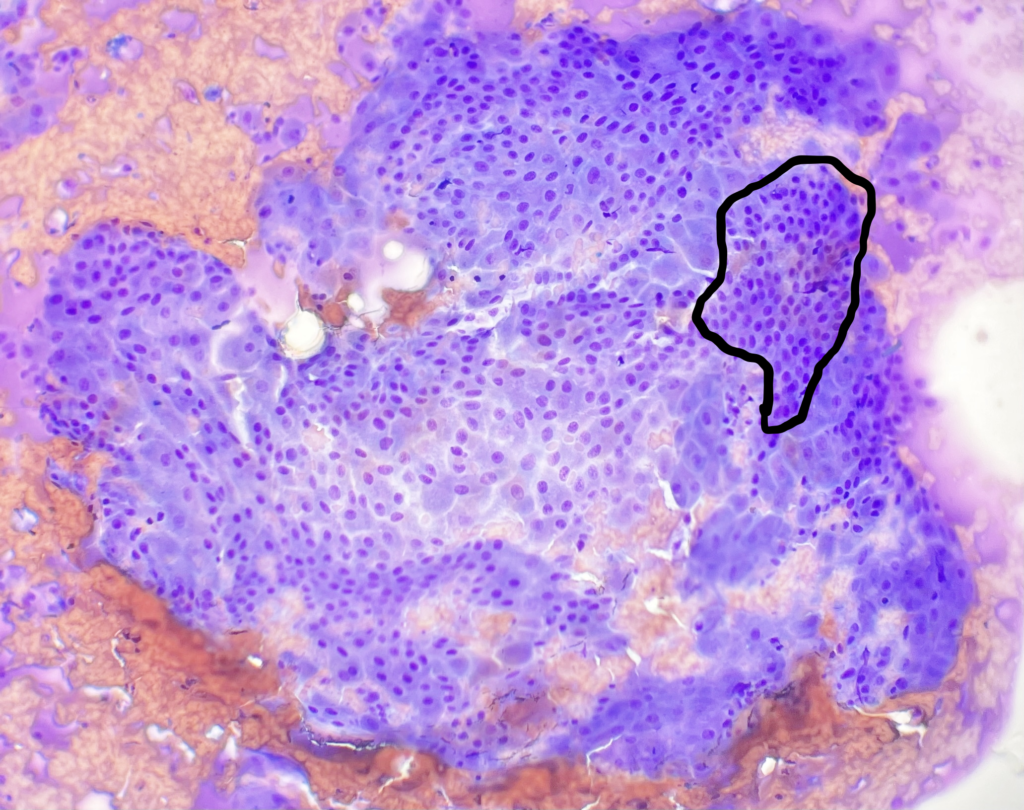
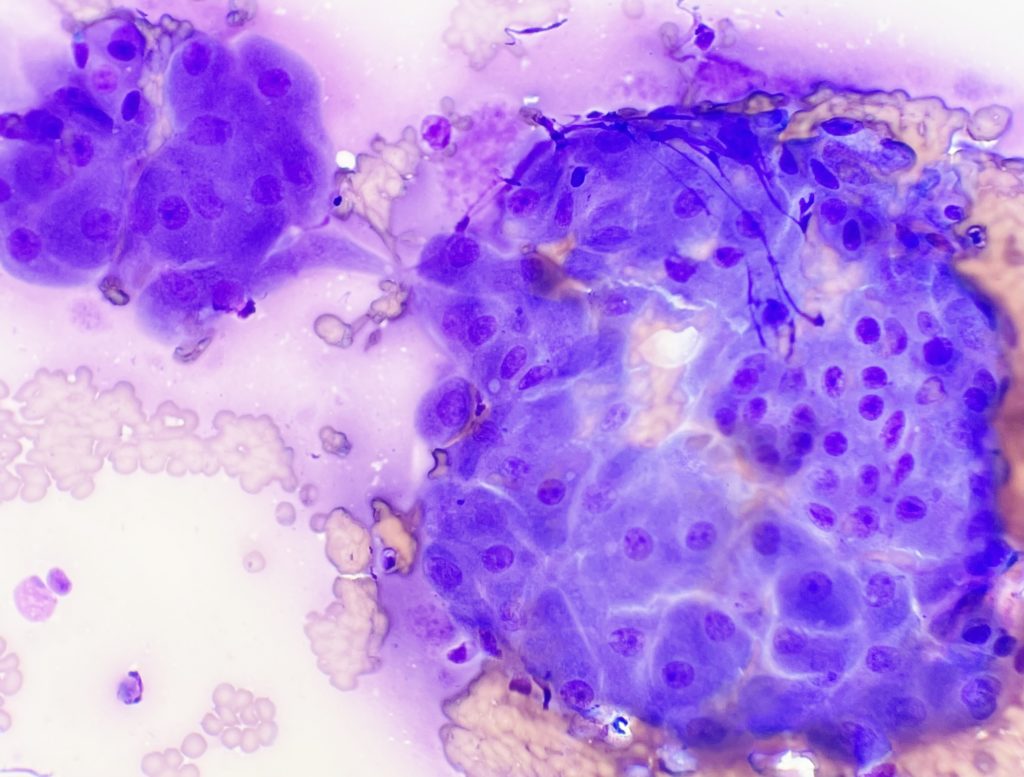
Aspirates tend to be moderately to highly cellular with variably sized, cohesive clusters of epithelium. The large cells resemble hepatocytes and tend to have distinct borders with a moderate to large amount of coarsely stippled, pinkish-blue cytoplasm. Nuclei are paracentral to eccentric and round to oval, with coarse chromatin and usually one or two variably distinct nucleoli. Typical features include moderate to low nuclear to cytoplasmic ratio, mild to moderate anisokaryosis (variability in nuclear size), and occasional bi-nucleation.
There are often “reserve cells”, which are essential basal cells, admixed with the more mature large hepatoid cells. The reserve cells are small polygonal cells with smaller nuclei and a high nuclear to cytoplasmic ratio.
Cytology is useful to confirm that a tumour is of circumanal gland origin. While most are benign/adenomas, histopathology is generally required to confirm malignant potential, if this step is clinically warranted.
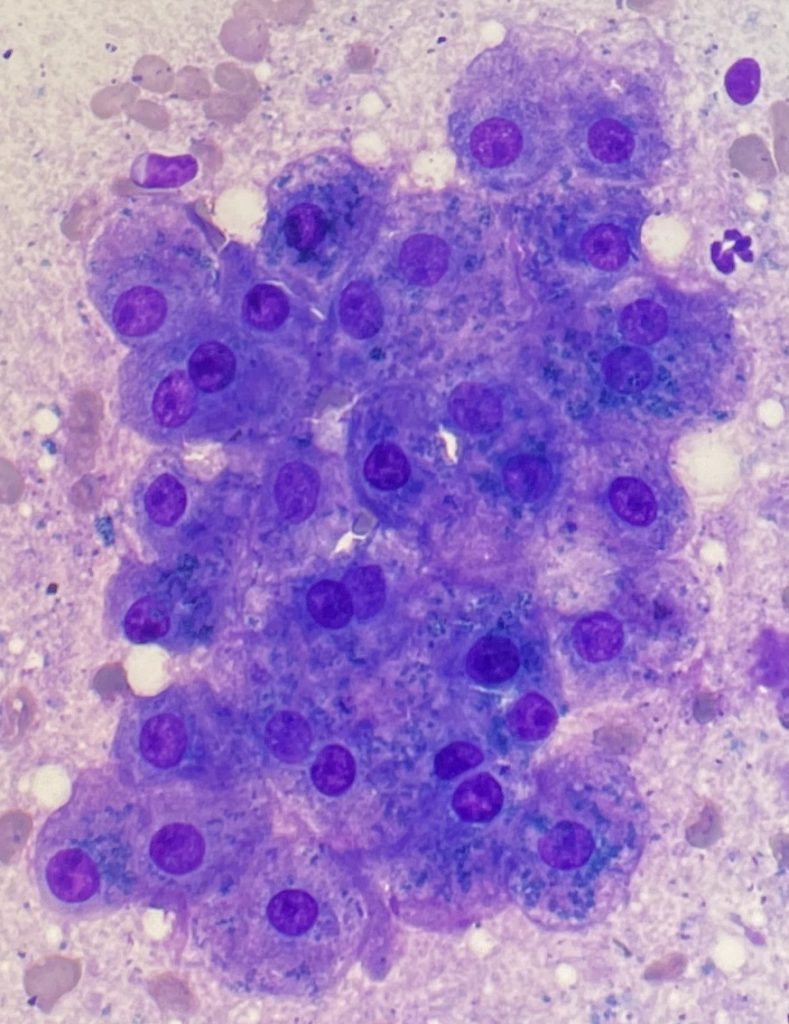
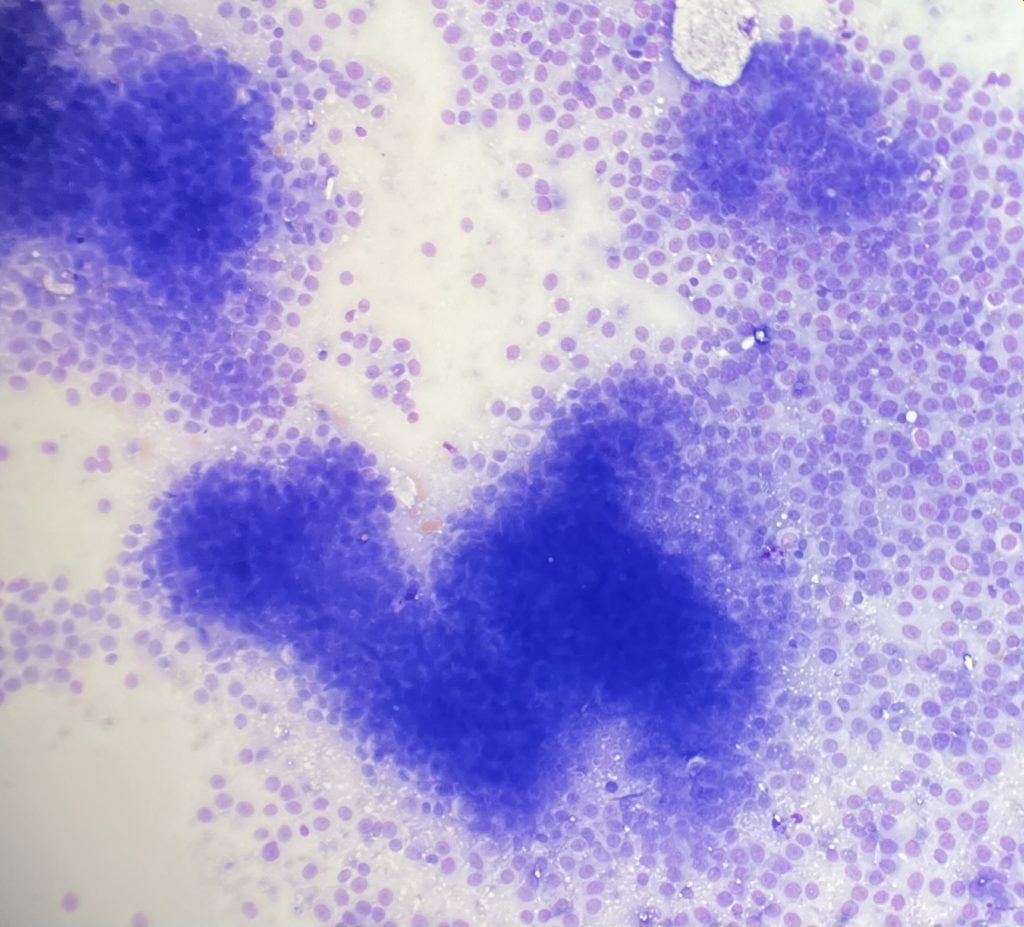
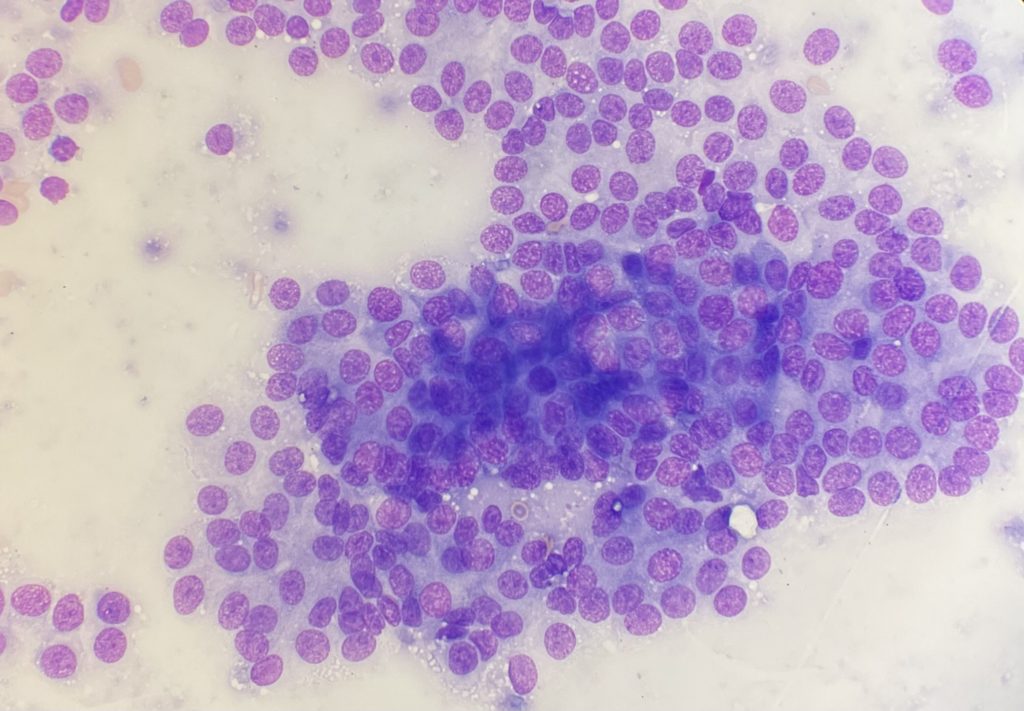
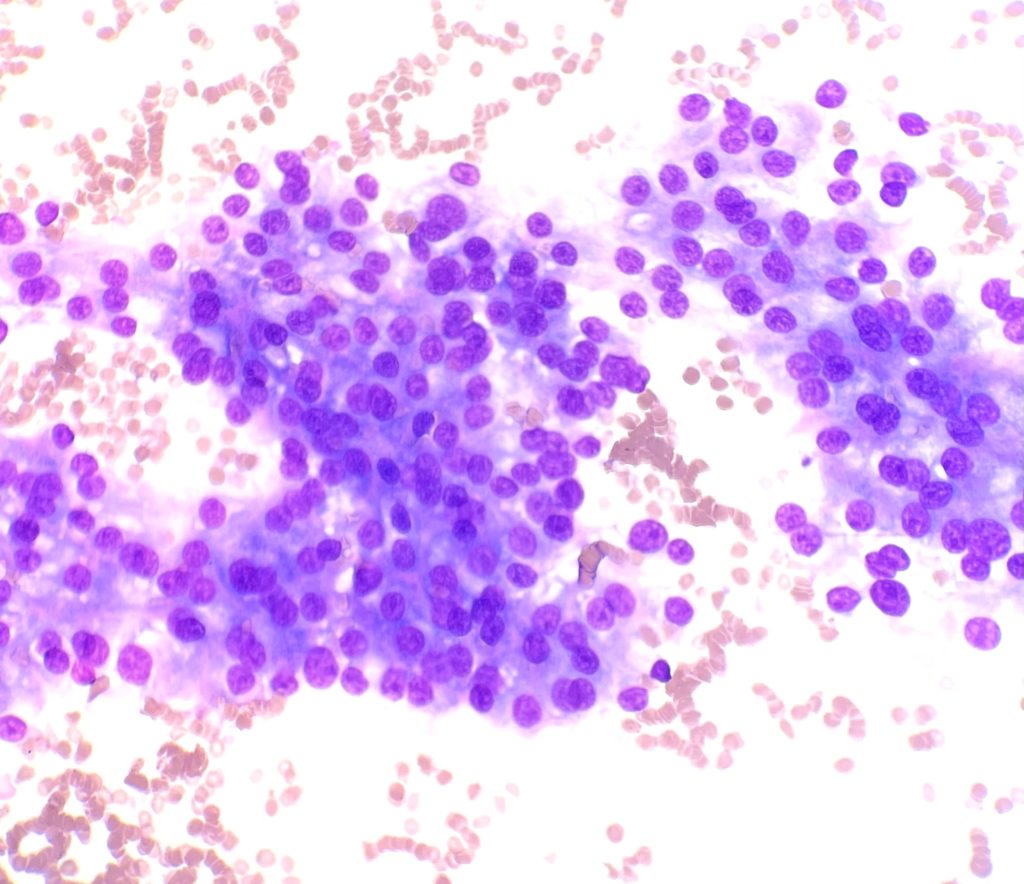
Anal sac apocrine gland adenocarcinomas arise from the anal sac epithelium and can invade surrounding structures. They are relatively common in the dog and rare in cats. According to some studies females are over-represented, but this is not a consistent finding across all studies.* Hypercalcaemia is a well-known paraneoplastic syndrome, but estimates of the frequency of this finding also vary. These tumours often metastasise to regional lymph nodes and sometimes distant sites. On cytology, the cells are usually found in clusters, which are often partially disrupted, displaying the “neuroendocrine appearance” of free nuclei surrounded by the cytoplasm of disrupted cells. When intact, the
cells are round or polygonal. The degree of atypia is variable (some are highly atypical), but most have few criteria of malignancy. The cells often have a uniform appearance with a moderate amount of pale to medium blue, sometimes vacuolated cytoplasm. Nuclei are round to oval with stippled chromatin and small, indistinct nucleoli.
If after all this comparison, these images and entities still look similar to you, don’t despair. You are always able to send the samples to us, and we’ll do our best to provide you with a diagnosis.